Belpomme D, Hardell L, Belyaev I, Burgio E, Carpenter DO. Thermal and non-thermal health effects of low intensity non-ionizing radiation: An international perspective. Environ Pollut. 2018 Nov;242(Pt A):643-658. doi: 10.1016/j.envpol.2018.07.019. Epub 2018 Jul 6. PMID: 30025338.
Abstract
Exposure to low frequency and radiofrequency electromagnetic fields at low intensities poses a significant health hazard that has not been adequately addressed by national and international organizations such as the World Health Organization. There is strong evidence that excessive exposure to mobile phone-frequencies over long periods of time increases the risk of brain cancer both in humans and animals. The mechanism(s) responsible include induction of reactive oxygen species, gene expression alteration and DNA damage through both epigenetic and genetic processes. In vivo and in vitro studies demonstrate adverse effects on male and female reproduction, almost certainly due to generation of reactive oxygen species. There is increasing evidence the exposures can result in neurobehavioral decrements and that some individuals develop a syndrome of “electro-hypersensitivity” or “microwave illness”, which is one of several syndromes commonly categorized as “idiopathic environmental intolerance”. While the symptoms are non-specific, new biochemical indicators and imaging techniques allow diagnosis that excludes the symptoms as being only psychosomatic. Unfortunately standards set by most national and international bodies are not protective of human health. This is a particular concern in children, given the rapid expansion of use of wireless technologies, the greater susceptibility of the developing nervous system, the hyperconductivity of their brain tissue, the greater penetration of radiofrequency radiation relative to head size and their potential for a longer lifetime exposure.
Final section of the paper: Public Health Implications of Human Exposure to EMFs
The incidence of brain cancer in children and adolescents has increased between 2000 and 2010 (Ostrom et al., 2015). Gliomas are increasing in the Netherlands (Ho et al., 2014), glioblastomas are increasing in Australia (Dobes et al., 2011) and England (Philips et al., 2018) and all brain cancers are increasing in Spain (Etxeberrua et al., 2015) and Sweden (Hardell and Carlberg, 2017). The latency period between initial exposure and clinical occurrence of brain cancer is not known but is estimated to be long. While not all reports of brain cancer rates show an increase, some do. The continually increasing exposure to EMFs from all sources may contribute to these increases. The prevalence of EHS is unknown, but various reports suggest that it is between 1 and 10% of the population (Hallberg and Oberfeld, 2006; Huang et al., 2018). Male fertility has been declining (Geoffroy-Siraudin et al., 2012; Levine et al., 2017). EMFs increase the risk of each of these diseases and others. Alzheimer’s disease is increasing in many countries worldwide and its association with ELF-EMF occupational exposure has been clearly demonstrated through several independent epidemiological studies (Davanipour and Sobel, 2009; Sobel et al., 1996; Qiu et al., 2004) and a meta-analysis of these studies (García et al., 2008). A recent meta-analysis (Huss et al., 2018) has reported an increased risk of amyotrophic lateral sclerosis in workers occupationally exposure to ELF-EMFs.
Safety limits for RF exposure have been based (until today) on the thermal effects of EMFs. But these standards do not protect people, particularly children, from the deleterious health effects of non-thermal EMFs (Nazıroğlu et al., 2013; Mahmoudabadi et al., 2015). Each of these diseases is associated with decrements in health and quality of life. Brain cancer patients often die is spite of some improvement in treatment, while EHS patients present with increased levels of distress, inability to work, and progressive social withdrawal. The ability for humans to reproduce is fundamental for the maintenance of our species.
The scientific evidence for harm from EMFs is increasingly strong. We do not advocate going back to the age before electricity or wireless communication, but we deplore the present failure of public health international bodies to recognize the scientific data showing the adverse effects of EMFs on human health. It is encouraging that some governments are taking action. France has removed WiFi from pre-schools and ordered Wi-Fi to be shut off in elementary schools when not in use (http://www.telegraph.co.uk.
It is urgent that national and international bodies, particularly the WHO, take this significant public health hazard seriously and make appropriate recommendations for protective measures to reduce exposures. This is especially urgently needed for children and adolescents. It is also important that all parts of society, especially the medical community, educators, and the general public, become informed about the hazards associated with exposure to EMFs and of the steps that can be easily taken to reduce exposure and risk of associated disease.
https://www.ncbi.nlm.nih.gov/pubmed/30025338
Excerpts
“In spite of a large body of evidence for human health hazards from non-ionizing EMFs at intensities that do not cause measureable tissue heating, summarized in an encyclopedic fashion in the Bioinitiative Report (www.bioinitiative.org), the World Health Organization (WHO) and governmental agencies in many countries have not taken steps to warn of the health hazards resulting from exposures to EMFs at low, non-thermal intensities, nor have they set exposure standards that are adequately health protective. In 2001 the International Agency for Research on Cancer (IARC, 2002), part of the WHO, declared ELF-EMFs to be “possibly carcinogenic to humans”, and in 2011 they made a similar declaration for RF-EMFs (Baan et al., 2011; IARC, 2013). The classification of RF-EMFs as a “possible” human carcinogen was based primarily on evidence that long-term users of mobile phones held to the head resulted in an elevated risk of developing brain cancer. One major reason that the rating was not at “probable” or “known” was the lack of clear evidence from animal studies for exposure leading to cancer. The US National Toxicology Program has released preliminary results of a study of long term exposure of rats to cell phone radiation which resulted in a statistically significant increase in brain gliomas, the same cancer found in people after long-term cell phone use, and schwannomas, a tumor similar to the acoustic neuroma also seen after intensive mobile phone use (Wyde et al., 2016). Similar results in rats have been reported in an independent study at the Ramazzini Institute with exposures similar to those from a mobile phone base station (Falcioni et al., 2018). This evidence, in conjunction with the human studies, demonstrates conclusively that excessive exposure to RF-EMF results in an increased risk of cancer. In light of this new evidence for cancer in rodents in response to prolonged exposure to mobile phone frequencies, the IARC rating should be raised at least to “probable” (Group 2A) if not “known” (Group 1).
Unfortunately the International EMF Project of the WHO, which is part of the Department of Public Health, Environment and Social Determinants of Health in Geneva, has consistently minimized health concerns from non-ionizing EMFs at intensities that do not cause tissue heating (WHO, 2014). In this regard WHO has failed to provide an accurate and human health-protective analysis of the dangers posed to health, especially to the health of children, resulting from exposure to non-thermal levels of electromagnetic fields. The Department of Public Health, Environment and Social Determinants of Disease takes its advice on the issues related to human health effects of non-ionizing EMFs from the International Commission on Non-ionizing Radiation Protection (ICNIRP). Almost all members of the core group preparing the new Environmental Health Criteria (EHC) document for the WHO are members of ICNIRP (Starkey, 2016; Hardell, 2017), a non-government organization (NGO) whose members are appointed by other members. In spite of recent efforts to control for conflicts of interest, ICNIRP has a long record of close associations with industry (Maisch, 2006). When queried as to why the WHO would take recommendations from such a group, WHO staff replied that ICNIRP is an official NGO which works closely with the WHO. Why this should exclude other scientific research groups and public health professionals is unclear, particularly since most members of ICNIRP are not active researchers in this field. We are particularly concerned that a new WHO EHC document on RF-EMFs is scheduled to be released soon, and that the members of the EHC Core Group and the individuals whose assistance has been acknowledged are known to be in denial of serious non-thermal effects of RF-EMFs in spite of overwhelming scientific evidence to the contrary (Starkey, 2016; Hardell, 2017).
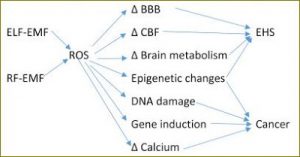
Others have dismissed the strong evidence for harm from ELF- and RF-EMFs by arguing that we do not know the mechanism whereby such low energetic EMFs might cause cancer and other diseases. We have definitive evidence that use of a mobile phone results in changes in brain metabolism (Volkow et al., 2011). We know that low-intensity ELF- and RF-EMFs generate reactive oxygen species (ROS), alter calcium metabolism and change gene expression through epigenetic mechanisms, any of which may result in development of cancer and/or other diseases or physiological changes (see www.bioinitiative.org for many references). We do not know the mechanisms behind many known human carcinogens, dioxins and arsenic being two examples. Given the strength of the evidence for harm to humans it is imperative to reduce human exposure to EMFs. This is the essence of the “precautionary principle”.”
“Based on case-control studies there was a consistent finding of increased risk for glioma and acoustic neuroma associated with use of mobile phones. Similar results were found for cordless phones in the Hardell group studies, although such use was not reported by the other study groups. The findings are less consistent for meningioma although somewhat increased risk was seen in the meta-analysis of ipsilateral mobile phone use. A longer follow-up time is necessary for this type of slow growing tumor.”
“There are other significant human health hazards of concern. There is strong animal and human evidence that exposure to RF-EMFs as well as ELF-EMFs reduces fertility in both males (reviewed by McGill and Agarwal, 2014) and females (Roshangar et al., 2014) … There is evidence that isolated human sperm exposed to RF-EMFs are damaged by generation of reactive oxygen species (Agarwal et al., 2009).”
“Exposure to RF-EMFs has been reported to increase neuropsychiatric and behavioural disorders (Johansson et al., 2010; Divan et al., 2012), trigger cardiac rhythm alteration and peripheral arterial pressure instability (Havas, 2013; Saili et al., 2015), induce changes in immune system function (Lyle et al., 1983; Grigoriev et al., 2010; Sannino et al., 2011, 2014) and alter salivary (Augner et al., 2010) and thyroid (Koyu et al., 2005; Mortavazi et al., 2009; Pawlak et al., 2014) function.”
“Children, and especially fetuses, are more vulnerable than adults for most environmental exposures (Sly and Carpenter, 2012) ….
Divan et al. (2008) reported that prenatal and to a lesser degree postnatal exposure to cell phones is associated with emotional and hyperactivity problems in 7-year old children. This finding was confirmed in a second replicative study involving different participants (Divan et al., 2012). Birks et al. (2017) used data from studies in five cohorts from five different countries (83,884 children) and concluded that maternal mobile phone use during pregnancy increased the risk that the child will show hyperactivity and inattention problems. A meta-analysis involving 125,198 children (mean age 14.5 years) reported statistically significant associations between access to and use of portable screen-based media devices (e.g. mobile phones and tablets) and inadequate sleep quality and quantity and excessive daytime sleepiness (Carter et al., 2016)….”
“The specific absorption rate (SAR)-based ICNIRP safety limits were established on the basis of simulation of EMF energy absorption using standardized adult male phantoms, and designed to protect people only from the thermal effects of EMFs. These assumptions are not valid for two reasons. Not only do they fail to consider the specific morphological and bioclinical vulnerabilities of children, but also they ignore the effects known to occur at non-thermal intensities….”
“There is a segment of the human population that is unusually intolerant to EMFs. The term “electromagnetic hypersensitivity” or “electrohypersensitivity (EHS)” to describe the clinical conditions in these patients was first used in a report prepared by a European group of experts for the European Commission (Bergqvist et al., 1997). Santini et al. (2001, 2003) reported similar symptoms occurring in users of digital cellular phones and among people living near mobile phone base stations ….
In summary it is the strong opinion of the authors that there is presently sufficient clinical, biological and radiological data emanating from different independent international scientific research groups for EHS, whatever its causal origin, to be acknowledged as a well-defined, objectively characterized pathological disorder.”
“Arguments used in the past to attempt to discount the evidence showing deleterious health effects of ELF-EMFs and RF-EMF exposure at non-thermal SAR levels were based on the difficulties encountered in understanding the underlying biological effects and the lack of recognized basic molecular mechanisms accounting for these effects. This is no longer the case. There are a number of well-documented effects of low intensity EMFs that are the mechanistic basis behind the biological effects documented above (www.bioinitiative.org). These include induction of oxidative stress, DNA damage, epigenetic changes, altered gene expression and induction including inhibition of DNA repair and changes in intracelluar calcium metabolism ….”

“EMFs at non-thermal intensities may interfere with other environmental stressors, showing an interplay of molecular pathways and resulting in either beneficial or detrimental health effects, depending on the nature and conditions of co-exposures (Novoselova et al., 2017; Ji et al., 2016). One example is the demonstration that RF-EMF exposure modulates the DNA damage and repair induced by ionizing radiation (Belyaev et al., 1993). Another example is the synergistic of exposure to lead and EMFs on cognitive function in children described above (Choi et al., 2017; Byun et al., 2017). These co-exposure factors should be considered when assessment of detrimental effects, including carcinogenicity, is performed.”
“Public Health Implications of Human Exposure to EMFs
The incidence of brain cancer in children and adolescents has increased between 2000 and 2010 (Ostrom et al., 2015). Gliomas are increasing in the Netherlands (Ho et al., 2014), glioblastomas are increasing in Australia (Dobes et al., 2011) and England (Philips et al., 2018) and all brain cancers are increasing in Spain (Etxeberrua et al., 2015) and Sweden (Hardell and Carlberg, 2017). The latency period between initial exposure and clinical occurrence of brain cancer is not known but is estimated to be long. While not all reports of brain cancer rates show an increase, some do. The continually increasing exposure to EMFs from all sources may contribute to these increases. The prevalence of EHS is unknown, but various reports suggest that it is between 1 and 10% of the population (Hallberg and Oberfeld, 2006; Huang et al., 2018). Male fertility has been declining (Geoffroy-Siraudin et al., 2012; Levine et al., 2017). EMFs increase the risk of each of these diseases and others. Alzheimer’s disease is increasing in many countries worldwide and its association with ELF-EMF occupational exposure has been clearly demonstrated through several independent epidemiological studies (Davanipour and Sobel, 2009; Sobel et al., 1996; Qiu et al., 2004) and a meta-analysis of these studies (García et al., 2008). A recent meta-analysis (Huss et al., 2018) has reported an increased risk of amyotrophic lateral sclerosis in workers occupationally exposure to ELF-EMFs.
Safety limits for RF exposure have been based (until today) on the thermal effects of EMFs. But these standards do not protect people, particularly children, from the deleterious health effects of non-thermal EMFs (Nazıroğlu et al., 2013; Mahmoudabadi et al., 2015). Each of these diseases is associated with decrements in health and quality of life. Brain cancer patients often die is spite of some improvement in treatment, while EHS patients present with increased levels of distress, inability to work, and progressive social withdrawal. The ability for humans to reproduce is fundamental for the maintenance of our species.
The scientific evidence for harm from EMFs is increasingly strong. We do not advocate going back to the age before electricity or wireless communication, but we deplore the present failure of public health international bodies to recognize the scientific data showing the adverse effects of EMFs on human health. It is encouraging that some governments are taking action. France has removed WiFi from pre-schools and ordered Wi-Fi to be shut off in elementary schools when not in use (http://www.telegraph.co.uk.news/2017/12/11/france-ipose-total-ban-mobile-phones-schools/). The State of California Department of Public Health has issued a warning on use of mobile phones and offered advice on how to reduce exposure (State of California, 2017). There are many steps that are neither difficult nor expensive that can be taken to use modern technology but in a manner that significantly reduces threats to human health.
It is urgent that national and international bodies, particularly the WHO, take this significant public health hazard seriously and make appropriate recommendations for protective measures to reduce exposures. This is especially urgently needed for children and adolescents. It is also important that all parts of society, especially the medical community, educators, and the general public, become informed about the hazards associated with exposure to EMFs and of the steps that can be easily taken to reduce exposure and risk of associated disease.”
https://www.sciencedirect.com/science/article/pii/S0269749118310157